 |
| Chickadees and Berries from Amanda Ilkov Snowflakes from Di Hiller Designs. |

Friday, 25 December 2015
Saturday, 5 December 2015
Spa or Bootcamp: A Case For Considering the Nervous System in Pain management

What was the difference between these two individuals? Mainly it was the state of their nervous systems. One had processed the fall, her injury, and was ready to get better. (How she did that so fast is amazing!) The other lady’s nervous system was still on guard, ready to pounce on anything that might be a threat.
So the question today is: How effective is therapy when the nervous system is so wound up? It’s pretty hard to do effective therapy if you can’t even touch the person!
One popular pain center described their program as a balance between a spa and a boot camp. You mostly saw the boot camp part in the gym; they would encourage people to push harder, keep going when they were tired, etc. And yes, their clients did see improvement...muscles were strengthened or stretched, there were increases in people’s endurance and the amount they could lift. Progress on charts. But looking at that program we just wondered, how much more progress could have been made if they emphasized the spa part too. If they took the time to lower people's nervous system response, and didn’t add to it by the “bootcamp” approach. What would have happened?
Our guess is that they would have seen longer term, sustainable changes. From what we’ve seen, pain and all that comes with it throws a huge amount of stress on our systems. Calming the nervous system down (so that it is not constantly on edge), opens the door for you to really benefit from any other therapy. This gives you a chance to integrate it, learn from it and move towards healing.
So, how can we do this? Well, there are many ways therapists can help to bring the nervous system back to a more balanced state. Here are just a few ideas:
- Calm the nervous system through “relaxation” methods: visualization, acupuncture, breathing exercises, yoga, laughter, massage, etc
- Create a relationship of trust with your client and validate their experiences. They don’t have to “prove” their pain, it’s just accepted.
- Reduce disability. Enabling your clients to do the things the need to do (teaching them a different way, changing the situation, etc) reduces the impact of the pain on their lives and in turn reduces the stress it places on their body.
- Address client's fears. Listen, educate, and try to come up with a solution. There are about a zillion new worries that come with pain and even acknowledging them can take some of the pressure off the body.
- Give your clients permission to rest. Often people in pain feel the need to keep pushing, which again adds more stress to the body.
If you’re a therapist we would love to hear what you do with your clients. What do you find works, and what doesn’t? If you have pain, what has worked for you? What are your thoughts?
You might have noticed on this blog we talk a lot about the nervous system. Well, this is why. We believe the process of learning to live well with pain can be only be enhanced by calming the nervous system.
It’s kind of funny that this little post about the “spa vs bootcamp” concept has been hanging out with our draft posts since the beginning. It asked a lot of questions, provided some speculation based on experience, but didn’t provide a lot of answers as to why the boot-camp approach wasn't enough. And then we went to a course that talked all about pain and the nervous system. Lightbulbs went off! In the new year we’ll carry on this discussion and talk a bit more about how the nervous system relates to pain and why it is so important to acknowledge this connection.
Sunday, 29 November 2015
The Importance of Self-Efficacy: A Mini-Post
Hello, and welcome to our second mini-post. We don't have a post to share every week, so we thought we would try sharing some mini-posts on the "in between" weeks. Today we have a quote to share with you.
One comment we've heard from many people in pain (an echoed in the literature) is the loss of control. The feeling that pain is making the decisions in life. Paying attention to self-efficacy (and looking for ways to foster it) is so important because it can help us regain that sense of power and control. Knowing that pain isn't making ALL the decisions in our lives can have a huge impact on both the experience of pain and on quality of life.
 |
| "I am not afraid of Storms, for I am learning how to sail my ship." ~ Louisa May Alcott |
One comment we've heard from many people in pain (an echoed in the literature) is the loss of control. The feeling that pain is making the decisions in life. Paying attention to self-efficacy (and looking for ways to foster it) is so important because it can help us regain that sense of power and control. Knowing that pain isn't making ALL the decisions in our lives can have a huge impact on both the experience of pain and on quality of life.
Tuesday, 17 November 2015
The Torn Blanket: How Pain Can Challenge Our Sense of Security
Recently I (Colleen) listened to an interview of Bill Moyers with Pema Chodron. In it they talk about security and the impact of challenging situations. When these situations arise, they can affect the parts of our lives that we see as stabilizing, the things that we use to create our sense of "ground." They discussed what happens when life removes this security and how we react to that sense of "groundlessness."
This lead to a discussion about our reaction to pain becoming part of our lives. (That's what happens when you write a blog with your friend!)
We think in many cases chronic pain forces us to examine the whole idea of security. For many people our grown-up “security blanket” includes our idea of health and our bodies’ capabilities. Our health is also inter-woven with other pieces of this blanket, like being able to provide for a family, do a certain job, or other parts how we define ourselves. The pieces that make up the blanket are different for everyone and depend a lot on individual beliefs and values.
When chronic pain (or disease) enters the picture it can change all this. It comes along and tears some pretty big holes in this nice secure blanket. This can be a scary place and a frustrating place. For some it can be a place of loss, for others a place of anger, or possibly confusion. All sorts of reactions can happen, and they can change over time. The parts that are torn and what parts are left will be different for every situation, and it is important to look at both parts.
So what do you do when you’re left holding a shredded blanket and looking at the gaps? We think that depends on individual beliefs and situations and the way each person handles obstacles in their life. We can't give you a one-size-fits-all action plan (as much as we would love to), but we can give you some things to think about
1. Be kind to yourself: This doesn't mean booking a $10,000 trip to your dream destination. It's more about treating yourself with kindness. Somebody once asked me (Colleen) to pretend it had been a friend in the accident, and to picture saying the things to her that I say to myself. I just started laughing and said "I would never say that!" It was a lesson that stuck - if I wouldn't say it to a friend, why is it okay to say to myself?
2. Recognize the losses and allow yourself permission to grieve. It really is okay to not be okay sometimes. It's okay to be sad, frustrated, angry, confused or crying. Acknowledging the losses doesn’t mean you are weak or unappreciative of the good things in life. In fact we think it takes a lot of courage to really stop and acknowledge what has changed. Allowing yourself to recognize that the changes in your life are significant is a huge part of creating the space to carry on. Try to find a balance - acknowledge the loss, but don't get stuck there.
3. Focus on the pieces that are still there. We know, we know, we can hear the groans through the computer. This isn't just one of those "glass half full" trivial comments people make. We realize this is so easy to say but not easy to do. We realize that sometimes it looks like the glass is totally empty and there isn't even a drop left. Even if there are big gaping holes in the blanket, there will also be pieces that are still whole. Look for these pieces, they might be hidden or frayed but they're still there. Celebrate them.
4. Learn to live with the holes and adjust your expectations. By keeping your standard bar at the same level it was when you were “better,” everything you do now could look like a failure in comparison. When really that’s not the case at all! By thinking this way, you are limiting yourself from recognizing successes in the present. It`s a fine balance between accepting the now and still leaving room for increased functioning, coping, and healing.
When all you can think about is making it through the day, it’s tough. But do yourself (or your clients) a favour, and focus on one tiny change at a time. You may feel like your security blanket is gone, but it will come back. It will look different than it once did, but it will still be beautiful.
Acknowledgement
Thank-you
to all the people who have shared their stories and wisdom with us.
If you're
interested here is the link to the interview:
http://pemachodronfoundation.org/videos/bill-moyers-on-faith-and-reason-with-pema-chodron/Saturday, 7 November 2015
Pain Superstar

Hello! One of the things we hope to do with this blog is encourage individuals to start to take back control of their lives from pain. We don`t have a post to share every week, so we thought we would try sharing some mini-posts on the "in between" weeks. Sometimes this might be a short youtube video that we feel explains something nicely, a quote or a resource. Today it is a `pain superstars' post where we highlight an example, story, or lesson from someone living with pain.
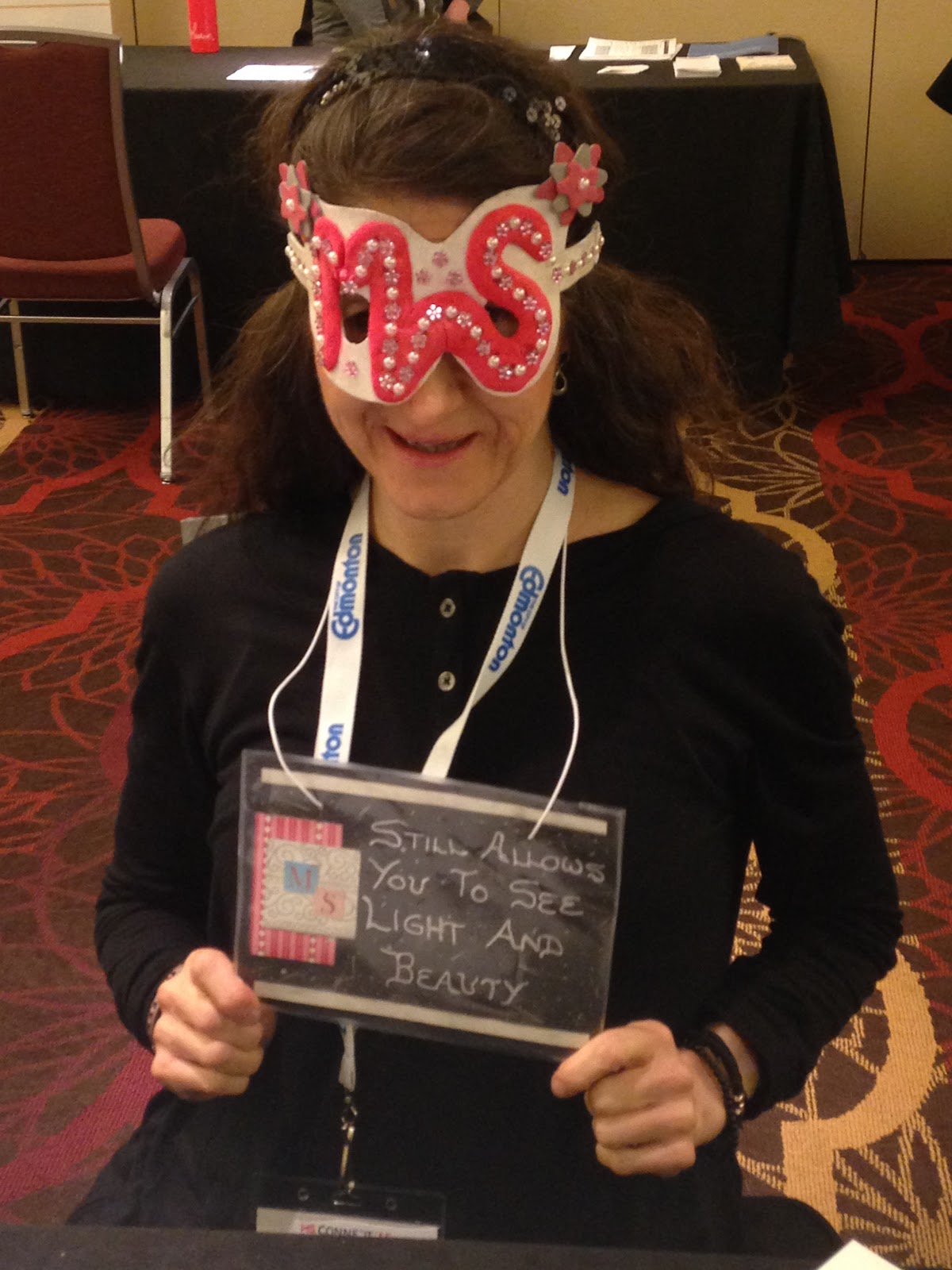 |
| Verbal consent was give to share this photo. |
I (Ashley) met this Pain Superstar at the Multiple Sclerosis Connections Conference in October 2015. She was making her rounds talking to as many people as possible, and she stopped to chat with me. She told me about how she had lived with pain for many years. She had 4 back surgeries before she was diagnosed with MS. She acknowledged the suffering she had experienced, but she was incredibly optimistic and positive. She explained that she had been asked in a recent art class to make a piece of art that described what MS meant to her. She made these glasses and this sign to show that to her, MS is something that “still allows you to see light and beauty”. She is a true example of living well with a chronic condition!
Tuesday, 3 November 2015
The Ability to Cope

How do you cope when your coping feels like it is gone? Sometimes all the pain, fatigue, stress, and everyday life challenges can feel like they pile up so high that one more thing is just too much. It’s like the figurative “straw that broke the camel’s back”. When we spend our lives close to that breaking point, it can leave us feeling easily annoyed, irritable, and frustrated with ourselves and others. It can feel like living in a really annoying itchy sweater, where every stimulus or stress becomes magnified, and so do our reactions. Sometimes our reactions add to the feeling of being broken, as we know that they are not in proportion to the problem and are different from how we would typically react to things.
All people go through this sometimes, with chronic pain or not. Tami Brady, a woman who has chronic fatigue syndrome and fibromyalgia, commented that "People are people. Some look like they have it all figured out. Trust me, they don’t. They are just good actors" (Brady, 2008). When chronic pain enters the picture and demands to be part of your life, there are bound to be times when you feel like you’ve been pushed past what you can take. This feeling could be brought on by too many stresses, not enough sleep, or a bad pain day.
These overwhelming symptoms can make it hard to deal with the other challenges life inevitably brings. One of the terms related to this concept is “frustration tolerance”, which is the ability to handle or deal with problems without getting upset (McCallister, 2013). It’s not surprising that when people develop chronic pain, their frustration tolerance changes. Their daily life stresses now include pain and the impact of pain. Other things that would not have been a problem before can suddenly become much more troubling.
When we asked our readers to send us their definition of pain, one response was "Pain hurts and affects everything. If I don't react how you think I should, please blame the pain, not me, or you."
"Please blame the pain, not me, or you." Such a short phrase but so very important. If you feel like you aren’t coping the way you should, like you’re too grumpy or irritable (or your loved one is), know that you are not just a grumpy, mean, short-tempered person. And like everything with pain, understanding helps. Understanding that pain affects our frustration tolerance and lessens our ability to deal with everyday stressors allows us to learn strategies to deal with it. After all, recognition is 50% of the solution, right?
What comes next is realizing that even though life/stress/pain/fatigue has you down at this moment, it doesn’t have to stay that way. You can feel this moment, and then move on from it. You can gather your resources and strength and get through this. There’s a song by Katherine Nelson that says “I was born to stand tall, I was born to face the wind, I was born to feel heart break and to heal again”. Even when it feels like we’re completely spent, and all our inner strength is gone, it’s still in there somewhere.
The key is learning how to access it. Those moments when life really has us down can be the hardest moments to remember how to find our strength. That’s why we love the idea Bronnie Thompson (2008) shared about “cue cards for coping.” The idea is that you identify the unique set of strategies that works best for you, and write them down on a card small enough to carry around with you. That way, when you need the strategies most, you will have a simple reminder to help you get through the worst times.
Sometimes it helps to have advice and reassurance for yourself in your own words. When it feels like no one truly understands how you feel, you might find your own words the most comforting. I (Ashley) had a difficult first pregnancy. After the baby was born, I knew I wanted to have another one, but I was afraid of what it would be like to be pregnant again. Over several months, I shared thoughts and strategies with my husband that I wanted him to remind me of if the next pregnancy was also difficult. Eventually he said “Why don’t you write all these thoughts down for yourself to read? You’ll believe your own words a lot better than you’ll believe me anyway”. There was some truth to what he said. I took his advice, and wrote myself a letter. Later on, when I did become pregnant for the second time, I read and re-read that letter whenever the challenges felt like too much to face.
So our suggestion is to take some time when you’re feeling okay, and think about what helps you cope. Write yourself a letter to explain it, or make some point form reminders on a card you can carry with you. Your set of strategies will be unique to you, but they might include things like deep breathing, relaxation exercises, music, calling a friend, heat or ice (ask your health care provider for advice on which one to try when), distraction in the form of a favourite movie, book, or video game, a you tube video that makes you giggle, massage, yoga, or any number of strategies to reduce the pain or improve your energy. Your health care provider can help you explore specific tools, but ultimately you know yourself best, and only you will know what combination of techniques works most effectively for you.
Acknowledgements:
All people go through this sometimes, with chronic pain or not. Tami Brady, a woman who has chronic fatigue syndrome and fibromyalgia, commented that "People are people. Some look like they have it all figured out. Trust me, they don’t. They are just good actors" (Brady, 2008). When chronic pain enters the picture and demands to be part of your life, there are bound to be times when you feel like you’ve been pushed past what you can take. This feeling could be brought on by too many stresses, not enough sleep, or a bad pain day.
These overwhelming symptoms can make it hard to deal with the other challenges life inevitably brings. One of the terms related to this concept is “frustration tolerance”, which is the ability to handle or deal with problems without getting upset (McCallister, 2013). It’s not surprising that when people develop chronic pain, their frustration tolerance changes. Their daily life stresses now include pain and the impact of pain. Other things that would not have been a problem before can suddenly become much more troubling.
When we asked our readers to send us their definition of pain, one response was "Pain hurts and affects everything. If I don't react how you think I should, please blame the pain, not me, or you."
"Please blame the pain, not me, or you." Such a short phrase but so very important. If you feel like you aren’t coping the way you should, like you’re too grumpy or irritable (or your loved one is), know that you are not just a grumpy, mean, short-tempered person. And like everything with pain, understanding helps. Understanding that pain affects our frustration tolerance and lessens our ability to deal with everyday stressors allows us to learn strategies to deal with it. After all, recognition is 50% of the solution, right?
What comes next is realizing that even though life/stress/pain/fatigue has you down at this moment, it doesn’t have to stay that way. You can feel this moment, and then move on from it. You can gather your resources and strength and get through this. There’s a song by Katherine Nelson that says “I was born to stand tall, I was born to face the wind, I was born to feel heart break and to heal again”. Even when it feels like we’re completely spent, and all our inner strength is gone, it’s still in there somewhere.
The key is learning how to access it. Those moments when life really has us down can be the hardest moments to remember how to find our strength. That’s why we love the idea Bronnie Thompson (2008) shared about “cue cards for coping.” The idea is that you identify the unique set of strategies that works best for you, and write them down on a card small enough to carry around with you. That way, when you need the strategies most, you will have a simple reminder to help you get through the worst times.
Sometimes it helps to have advice and reassurance for yourself in your own words. When it feels like no one truly understands how you feel, you might find your own words the most comforting. I (Ashley) had a difficult first pregnancy. After the baby was born, I knew I wanted to have another one, but I was afraid of what it would be like to be pregnant again. Over several months, I shared thoughts and strategies with my husband that I wanted him to remind me of if the next pregnancy was also difficult. Eventually he said “Why don’t you write all these thoughts down for yourself to read? You’ll believe your own words a lot better than you’ll believe me anyway”. There was some truth to what he said. I took his advice, and wrote myself a letter. Later on, when I did become pregnant for the second time, I read and re-read that letter whenever the challenges felt like too much to face.
So our suggestion is to take some time when you’re feeling okay, and think about what helps you cope. Write yourself a letter to explain it, or make some point form reminders on a card you can carry with you. Your set of strategies will be unique to you, but they might include things like deep breathing, relaxation exercises, music, calling a friend, heat or ice (ask your health care provider for advice on which one to try when), distraction in the form of a favourite movie, book, or video game, a you tube video that makes you giggle, massage, yoga, or any number of strategies to reduce the pain or improve your energy. Your health care provider can help you explore specific tools, but ultimately you know yourself best, and only you will know what combination of techniques works most effectively for you.
Acknowledgements:
Rope image courtesy of scottchan at FreeDigitalPhotos.net
References:
McCallister, M.J. (2013). Institute for Chronic Pain: Understanding Chronic Pain. Retrieved from http://www.instituteforchronicpain.org/understanding-chronic-pain/complications/depression on November 2, 2015
Thompson, B. (2008). HealthSkills: Cue Cards for Coping. Retrieved from https://healthskills.wordpress.com/2008/10/15/cue-cards-for-coping/ on November 2, 2015
Saturday, 24 October 2015
It's All About The Nervous System: What We Learned Last Weekend

It was so exciting for us to be able to attend a workshop meant specifically for occupational therapists. We believe that there needs to be a greater occupational therapy (OT) presence in pain management. After all, research is growing to support the concept that the primary reason people seek help for pain isn’t the pain itself, it’s the impact on their lives (Crombez, Eccleston, Van Damme, Vlaeyen & Karoly, 2012). Occupational therapists are all about function and helping people to engage in meaningful activities. Sounds like a good fit! Pain management gives us an excellent opportunity to look at the whole picture of what is going on in a person’s life and use a wide variety of OT skills. As a result we can have a profound impact in helping people navigate the world of pain and begin to reclaim their lives.
An essential key point we took from this workshop is that management of persistent pain is all about calming the nervous system. Persistent pain is not necessarily an “issue in the tissue” (although it may start out that way), but a symptom of a wound-up nervous system. We may not be able to eliminate the pain, but we can definitely change the inputs that the nervous system receives. By calming down the nervous system, we can begin to increase function and over time reduce the pain response. And that’s really exciting!
This workshop combined the concept of calming the nervous system with the Canadian Model of Occupational Performance (if you’re curious about the model, see our “About Us” page). Together, these two concepts helped us create a solid framework and foundation for a deeper understanding of pain. This was an excellent way to solidify and connect the concepts we have come to understand from our education, personal experiences, and continued learning, while at the same time building on this knowledge.
As well as impacting us professionally, this workshop also had a personal impact. It helped both of us as we continue to make sense of our own lives, and how we can help others do the same. At a few points in the workshop, we turned to each other and said “it all makes sense now!” One of us even cried as a particular statement hit very close to home, so maybe going to the workshop was actually a form of therapy for us.
Overall, we are so glad we went, and we’re excited to share what we’ve learned with you. The workshop made so much sense in terms of what we each have experienced in our own lives and made us even more excited about sharing what we’re learning through this blog. You’ll definitely see concepts from this workshop in our future blog posts. Stay tuned for more!
Acknowledgment:
Diagram by Ashley and Colleen at Reclaiming Life. Graphics used are from freepik.com.
References
Crombez, G., Eccleston, C., Van Damme, S., Vlaeyen, J.W.S., & Karoly, P. (2012). Fear-avoidance model of chronic pain: The next generation. The Clinical Journal of Pain. Volume 28 (6), 475-483.
Wednesday, 21 October 2015
Meet and Greet
Hi Everyone,
We are so excited to see that people are reading (and hopefully enjoying) our blog! We would love to get to know you and find out what topics you would like to see covered in the future. If you could take a moment to fill this survey out we would greatly appreciate it!
Thanks so much for your time,
Ashley and Colleen
P.S. Only the first two questions show up. Please scroll down for the other two. Thanks!
We are so excited to see that people are reading (and hopefully enjoying) our blog! We would love to get to know you and find out what topics you would like to see covered in the future. If you could take a moment to fill this survey out we would greatly appreciate it!
Thanks so much for your time,
Ashley and Colleen
P.S. Only the first two questions show up. Please scroll down for the other two. Thanks!
Tuesday, 13 October 2015
Your Brain is Trying to Protect You, Part Three: More Tools

1. Knowledge: Understanding what is happening inside the body
One important way to begin to address fear avoidance is with knowledge. Some people with pain spend a lot of time learning about their condition through books, the internet, and other sources. The information they find may or may not be accurate, and this should be considered. Other people in pain may avoid the topic, wanting to spend as little time thinking and focusing on it as possible. Whatever the case, we believe that the person in pain is the “expert” on their own experience. Health care providers can be “experts” in current evidence, theory, and knowledge around pain, and sharing this information with clients can be extremely helpful.
The knowledge that is provided can take many different forms:
The knowledge that is provided can take many different forms:
-What is happening inside the body?
-Which movements are good versus which ones could be harmful?
-Which activities are safe and which are unsafe?
-What does pain mean? Is it causing damage, or not?
-Coping strategies, techniques, and resources that are available.
Using knowledge and education to address fear avoidance sounds obvious, but there are many factors that affect the the outcome of education. For instance, a 2003 study on using education to address fear avoidance suggested that, as expected, people who were avoiding tasks because of fear of pain benefited from fear avoidance based physical therapy. What the authors didn’t expect was that the same education could actually lower clinical outcomes in people who they considered “confronters”, meaning people who tended not to try to avoid pain (George, Fritz, Bialosky & Donald, 2003). We interpret this to mean that it is essential for the clinician to understand the client’s current beliefs about their pain in order to determine what kind of information might be helpful to the client.
Using knowledge and education to address fear avoidance sounds obvious, but there are many factors that affect the the outcome of education. For instance, a 2003 study on using education to address fear avoidance suggested that, as expected, people who were avoiding tasks because of fear of pain benefited from fear avoidance based physical therapy. What the authors didn’t expect was that the same education could actually lower clinical outcomes in people who they considered “confronters”, meaning people who tended not to try to avoid pain (George, Fritz, Bialosky & Donald, 2003). We interpret this to mean that it is essential for the clinician to understand the client’s current beliefs about their pain in order to determine what kind of information might be helpful to the client.
2. Self-Efficacy: Believing that you can do something about the pain
Another essential tool is self-efficacy, a term that came from Bandura, a prominent psychologist in the 1990s. Some people may wonder - why talk about psychology when the problem is physical pain? The answer is that human beings are complex, and our minds and bodies impact each other. To put it succinctly, “chronic pain is inherently both a medical and a psychological condition – what healthcare providers call a biopsychosocial condition” (McCallister, 2013).
So what is self-efficacy? The textbook definition of self-efficacy is: “one’s belief about one’s ability to perform behaviors that should lead to expected outcomes” (Weiten, 2004). Basically, when it comes to pain, self-efficacy is the belief that you can manage the pain and continue living your life. Self-efficacy is essential to overcoming the effects that pain can have on everyday life. When people truly believe that they can do the things that are important to them and enjoy activities despite pain, they are well on their way to reclaiming their lives.
The great news is that health care providers can help people develop self-efficacy. One way is through information, as we described above. As Sandy Hilton explained, “when a person isn't afraid they are going to hurt themselves it allows them to act with more self-efficacy” (Hilton & Blickenstaff, 2015). So health care providers can encourage people to build self-efficacy by providing information about what movements and activities are safe to try. Once the person begins to try things and have success with them, the feeling of “I can do this” is reinforced.
Health care providers can also enhance self-efficacy simply by choosing their language and focus carefully. Sandy Hilton described this as “looking for opportunities instead of dysfunction in the way we describe things with patients.” By keeping our language ability-focused rather than impairment-focused, we emphasize people’s strengths, and reinforce that they can use these strengths to their advantage in managing pain (Hilton & Blickenstaff, 2015).
If you are a person in pain, look for health care providers who encourage and support you to develop your own strengths and abilities in managing your condition. Also, keep an eye out for ways to foster this empowerment in your own life.
3. Re-introduce movements and activities: Gradually taking activities back from the thief
Re-introducing movements that have become worrisome is basically hypothesis testing and rewiring the connections in the brain. In a way it is creating that sense of safety for the body to progress. It is saying “You know that big, bad thing you're afraid of? Well maybe it just isn’t so scary as you think. Maybe you can deal with it.” There are different ways to create that sense of safety so there is room to increase activities, but today we are specifically going to look at graded exposure. This part of our post will be geared more toward clinicians, as it will be detailed about the specific therapy approaches. Through graded exposure the hypothesis of “If I do this movement, then I will cause pain or harm” is being tested.
It’s important to note that graded exposure is different from graded activity. Both have a role in pain management, but graded exposure specifically has a role in looking at fear avoidance behaviour. Graded activity is where you choose one specific action, and gradually increase the difficulty level (intensity, duration, speed, etc) to increase your ability (strength, coordination, and skill). Graded exposure is where you look at the activities you’ve avoided because of fear of pain, and work from the “least scary” task to the “most scary”, to increase your confidence.
For example, if you’ve been avoiding carrying groceries in from the car, graded activity would be starting with a box of cereal, then gradually building up to heavier grocery items. The goal would be to build up muscle strength so you can physically carry all the necessary groceries. Graded exposure addresses the emotional and psychological side more than the physical side. For example, if your specific fear is that carrying the groceries will result in injuring yourself further, being in excruciating pain, or not being able to go to work the next day, etc, then graded exposure addresses this fear. In graded exposure, you are not necessarily grading the specific activity, but grading which activities you’ll try, in what order. You would grade the exposure by starting with tasks that cause less anxiety and working up to tasks that have more fear attached to them.
You might ask - what if my fear is a worsening of pain, and the fear comes true? Prior to beginning graded exposure, the clinician would help the client develop strategies for addressing these situations. Then, even if the hypothesis is proven true, the client is able to cope, and confidence still builds. We would also anticipate that often the consequence may not be as severe as the client fears (for example, if the client fears they will “break their back” lifting the groceries, the reality is they may find their pain increases temporarily, but they are extremely unlikely to actually fracture a vertebra).
When we first starting learning about graded exposure, we both wondered “why would anyone ever want to do this? It sounds awful and hard”. We’ve learned that the motivation for this particular method of re-introducing movements and activities often comes when people recognize that fear is affecting what they’re able to do, and they want to take back the control. This approach is also different from “flooding”, which is what some people associate with exposure therapy. In flooding, people do things no normal person would do - like climbing in dumpsters if they are afraid of germs. Instead, this approach focuses on realistic everyday activities.
When deciding what activities to start with and what order to try activities it is critical to choose an activity that is both physically doable and emotionally achievable, and this is where the health care provider’s expertise and encouragement come in. The first consideration is the safety of the task, and whether the person believes it is safe. The second consideration is how realistic the task is - it has to be a task that the client can achieve. By starting with something that is achievable it creates that confidence and momentum to continue forward. Together both of these mean start small. Start with something that is just a tiny bit scary. Don’t give a grade one kid the New York Times and expect them to love reading. Instead you start with books that are at their reading level and gradually build up, and one day they just might grow up to be someone who loves the New York Times.
All these tools work together
To summarize, we will return to the example of the gentleman with back pain from our previous two posts. He was able to find success in regaining activities because of the combination of tools that met his individual needs. His doctor began by establishing trust and a working relationship. Then the doctor provided education on back pain and how “hurt does not always equal harm”, and movement can actually help improve symptoms. Next the doctor focused on building his self-efficacy by empowering him to realize that the tools he needed were within his reach. Then they discussed specific movements and activities that he had become hesitant about, even though they were important in his life. The doctor helped him understand how to start small in approaching these activities, and how to build on each success. The doctor encouraged him when needed and celebrated with him as he regained these activities. These tools together acted as a shield, protecting the man’s daily activities from the impact of pain.
Each person’s story is different, and in real life it may not be as simple as a person approaching their doctor and finding straightforward answers about how to implement these tools. It may be a different kind of health care provider, or a whole team of providers who do this. It may not be a linear process, and these are only a few of the many tools that can be used. The pain fear avoidance model does not address all possible factors that might be involved in a person’s pain experience. We’ve simplified it for the purposes of this post. But even though each person’s journey and tools will be different, we hope you have found this overview helpful in beginning to understand how health care providers can support people in reclaiming their lives.
Acknowledgment:
Another essential tool is self-efficacy, a term that came from Bandura, a prominent psychologist in the 1990s. Some people may wonder - why talk about psychology when the problem is physical pain? The answer is that human beings are complex, and our minds and bodies impact each other. To put it succinctly, “chronic pain is inherently both a medical and a psychological condition – what healthcare providers call a biopsychosocial condition” (McCallister, 2013).
So what is self-efficacy? The textbook definition of self-efficacy is: “one’s belief about one’s ability to perform behaviors that should lead to expected outcomes” (Weiten, 2004). Basically, when it comes to pain, self-efficacy is the belief that you can manage the pain and continue living your life. Self-efficacy is essential to overcoming the effects that pain can have on everyday life. When people truly believe that they can do the things that are important to them and enjoy activities despite pain, they are well on their way to reclaiming their lives.
The great news is that health care providers can help people develop self-efficacy. One way is through information, as we described above. As Sandy Hilton explained, “when a person isn't afraid they are going to hurt themselves it allows them to act with more self-efficacy” (Hilton & Blickenstaff, 2015). So health care providers can encourage people to build self-efficacy by providing information about what movements and activities are safe to try. Once the person begins to try things and have success with them, the feeling of “I can do this” is reinforced.
Health care providers can also enhance self-efficacy simply by choosing their language and focus carefully. Sandy Hilton described this as “looking for opportunities instead of dysfunction in the way we describe things with patients.” By keeping our language ability-focused rather than impairment-focused, we emphasize people’s strengths, and reinforce that they can use these strengths to their advantage in managing pain (Hilton & Blickenstaff, 2015).
If you are a person in pain, look for health care providers who encourage and support you to develop your own strengths and abilities in managing your condition. Also, keep an eye out for ways to foster this empowerment in your own life.
3. Re-introduce movements and activities: Gradually taking activities back from the thief
Re-introducing movements that have become worrisome is basically hypothesis testing and rewiring the connections in the brain. In a way it is creating that sense of safety for the body to progress. It is saying “You know that big, bad thing you're afraid of? Well maybe it just isn’t so scary as you think. Maybe you can deal with it.” There are different ways to create that sense of safety so there is room to increase activities, but today we are specifically going to look at graded exposure. This part of our post will be geared more toward clinicians, as it will be detailed about the specific therapy approaches. Through graded exposure the hypothesis of “If I do this movement, then I will cause pain or harm” is being tested.
It’s important to note that graded exposure is different from graded activity. Both have a role in pain management, but graded exposure specifically has a role in looking at fear avoidance behaviour. Graded activity is where you choose one specific action, and gradually increase the difficulty level (intensity, duration, speed, etc) to increase your ability (strength, coordination, and skill). Graded exposure is where you look at the activities you’ve avoided because of fear of pain, and work from the “least scary” task to the “most scary”, to increase your confidence.
For example, if you’ve been avoiding carrying groceries in from the car, graded activity would be starting with a box of cereal, then gradually building up to heavier grocery items. The goal would be to build up muscle strength so you can physically carry all the necessary groceries. Graded exposure addresses the emotional and psychological side more than the physical side. For example, if your specific fear is that carrying the groceries will result in injuring yourself further, being in excruciating pain, or not being able to go to work the next day, etc, then graded exposure addresses this fear. In graded exposure, you are not necessarily grading the specific activity, but grading which activities you’ll try, in what order. You would grade the exposure by starting with tasks that cause less anxiety and working up to tasks that have more fear attached to them.
You might ask - what if my fear is a worsening of pain, and the fear comes true? Prior to beginning graded exposure, the clinician would help the client develop strategies for addressing these situations. Then, even if the hypothesis is proven true, the client is able to cope, and confidence still builds. We would also anticipate that often the consequence may not be as severe as the client fears (for example, if the client fears they will “break their back” lifting the groceries, the reality is they may find their pain increases temporarily, but they are extremely unlikely to actually fracture a vertebra).
When we first starting learning about graded exposure, we both wondered “why would anyone ever want to do this? It sounds awful and hard”. We’ve learned that the motivation for this particular method of re-introducing movements and activities often comes when people recognize that fear is affecting what they’re able to do, and they want to take back the control. This approach is also different from “flooding”, which is what some people associate with exposure therapy. In flooding, people do things no normal person would do - like climbing in dumpsters if they are afraid of germs. Instead, this approach focuses on realistic everyday activities.
When deciding what activities to start with and what order to try activities it is critical to choose an activity that is both physically doable and emotionally achievable, and this is where the health care provider’s expertise and encouragement come in. The first consideration is the safety of the task, and whether the person believes it is safe. The second consideration is how realistic the task is - it has to be a task that the client can achieve. By starting with something that is achievable it creates that confidence and momentum to continue forward. Together both of these mean start small. Start with something that is just a tiny bit scary. Don’t give a grade one kid the New York Times and expect them to love reading. Instead you start with books that are at their reading level and gradually build up, and one day they just might grow up to be someone who loves the New York Times.
All these tools work together
To summarize, we will return to the example of the gentleman with back pain from our previous two posts. He was able to find success in regaining activities because of the combination of tools that met his individual needs. His doctor began by establishing trust and a working relationship. Then the doctor provided education on back pain and how “hurt does not always equal harm”, and movement can actually help improve symptoms. Next the doctor focused on building his self-efficacy by empowering him to realize that the tools he needed were within his reach. Then they discussed specific movements and activities that he had become hesitant about, even though they were important in his life. The doctor helped him understand how to start small in approaching these activities, and how to build on each success. The doctor encouraged him when needed and celebrated with him as he regained these activities. These tools together acted as a shield, protecting the man’s daily activities from the impact of pain.
Each person’s story is different, and in real life it may not be as simple as a person approaching their doctor and finding straightforward answers about how to implement these tools. It may be a different kind of health care provider, or a whole team of providers who do this. It may not be a linear process, and these are only a few of the many tools that can be used. The pain fear avoidance model does not address all possible factors that might be involved in a person’s pain experience. We’ve simplified it for the purposes of this post. But even though each person’s journey and tools will be different, we hope you have found this overview helpful in beginning to understand how health care providers can support people in reclaiming their lives.
Acknowledgment:
Diagram by Ashley and Colleen at Reclaiming Life. Graphics used are from Vector Characters.
References
George, S.Z., Fritz, J.M., Bialosky, J.E., & Donald, D.A. (2003). The effect of a fear-avoidance-based physical therapy intervention for patients with acute low back pain: results of a randomized clinical trial. SPINE, Volume 28 (23), 2551-2560.
Hilton, S., Blickenstaff, C. (Physical Therapists). (2015, June 9). Pain science and sensibility Episode 1: Self-efficacy and fear of movement in chronic back pain. [Audio podcast]. Retrieved from http://ptpodcast.com/pain-science-and-sensibility-episode-1-self-efficacy-and-fear-of-movement-in-chronic-back-pain/
McCallister, M.J. (2013). Institute for Chronic Pain Blog: Fear-Avoidance of Pain. Retrieved from http://www.instituteforchronicpain.org/blog/fear-avoidance-pain/ on August 31, 2015.
Weiten, W. (2004). Psychology themes & variations. California: Thomson Wadsworth.
Wednesday, 23 September 2015
Your Brain is Just Trying to Protect You, Part Two: What Can You Do?

Today we are going to learn about the shield built by our fictional gentleman and his doctor. The tools they used to build this shield consisted of: respecting his body, therapeutic relationship, knowledge, self-efficacy and re-introducing activities. Some of the tools were focused on mitigating the effect of pain and fear on current and future behaviours. They also had tools that were more designed to help them deal with the thief and reclaim the activities that he had already taken. Their goal wasn’t to relieve all the pain, but instead to reclaim his life by putting him back in charge.
It’s important to note that none of these tools work as well
in isolation as they do together. And that not every person will benefit from
every tool. Rainville et al. (2011) talked about how there are multiple factors
behind fear avoidance behaviour. There is misinformation (e.g. I will do harm
because someone said so), learned behaviour (e.g. this hurt, so I avoid it),
and emotional behaviour (e.g. fear driven). Recognizing these factors can give
a good starting point to identify which tools may be most helpful.
The Tools
1.) Respecting your body: Permission to not be okay
So often it is easy to fall into the “I shouldn’t feel like
this” mentality. A good first step is to allow yourself the courtesy to respect
whatever you are feeling. Part of this is simply acknowledging these concerns
and fears. It’s respecting the fact that pain avoidance is a logical reaction
and that it’s not a sign of weakness. Recently we both attended Bronnie
Lennox-Thompson’s course on Graded Exposure for Pain Avoidance. One of the
things she said during the course that really resonated with us was the idea of
creating space for the fear around the task and doing it anyways. The goal isn’t
to logic away the fear or ignore it but rather to acknowledge it and respect
that it is there. It’s something that happened with the injury that you have to
treat just as you do the physical symptoms.
2.) Therapeutic Relationship: Meet people where they are
The creation of a relationship between the practitioner and
client is one of the first things that happens when a person seeks treatment.
This relationship can have a huge impact on the outcome. Because it is so
important we think it is worth it to step back and examine this relationship
for a moment. If you’re reading this as a health care provider hopefully the
explanation of this tool will give you a basis for understanding the importance
of how you interact with clients. If you’re reading this as a person in pain or
a family member, this can help you understand why it’s beneficial for you to
find health care providers who really connect with you.
There are many factors that go into creating a strong
therapeutic relationship. The way these factors interact may depend on
the two people involved. One if the key factors that is common across
situations is the idea of validating the person’s experience; allowing the
client to have a voice and be heard and to feel safe expressing their
experience, questions and concerns. Pain is often a sensitive issue
and like any “invisible illness” people can often feel judged. People in pain
may be bombarded with societal messages such as “your pain is not real” or
“suck it up and deal with it.” They might come feeling like they have to defend
the pain or justify their behaviour. They really need to know that their
health care provider believes them and is on their side. They need to be able
to trust that their concerns are valued, and that their questions won’t be
minimized. A supportive health care provider will look for the reason behind
the concerns a patient decides to voice.
The person in pain also needs to know and trust that the
health care provider knows what they’re talking about. A client once told a
therapist “you’re like a friend who comes, but is full of knowledge.” Having
this type of therapeutic relationship can be the starting point that all the
other tools build on. A study on therapeutic alliance in the context of
treating lower back pain suggested that “factors related to the therapist
seemed to be as important as the therapy in pain modulation, and their
interaction may produce substantive clinical benefits”. The authors of the
study went further to say” The effect of accepted interventions can be improved
when clinicians interact positively with their patients” (Fuentes et al). A
good relationship is key to allowing any of the next tools to be effective.
The two tools discussed in this post (respecting the body
and therapeutic relationship) are the foundation for the other tools we will
discuss. Next post, we’ll go into detail about knowledge, self-efficacy, and
re-introducing movements. We hope this overview will be helpful to you as you
begin to build a shield with your own tools.
Acknowledgements
Diagram by Ashley and Colleen at Reclaiming Life. Graphics from Freepik.com (man, grocery basket, doctor, shield).
References
Fuentes, J., Armijo-Olivo, S., Funabashi, M., Miciak, M., Dick, B., Warren, S….Gross, D.P., (2014). Enhanced Therapeutic Alliance Modulates Pain Intensity and Muscle Pain Sensitivity in Patients With Chronic Low Back Pain: An Experimental Controlled Study. Physical Therapy, 94(4), 477-489.
Rainville, J., Smetts, R.J.E.M., Bendix, T., Tveito, T.H., Poiraudeau, S., & Indahl, A.J., (2011). Fear-avoidance beliefs and pain avoidance in low back pain. The Spine Journal, 11, 895-903.
Subscribe to:
Posts (Atom)