This post will be a little different from our typical chronic pain post. This is a real-life story about a woman who was able to use strategies based on pain theories to minimize disability from her pain. This post will bring together points that have been made throughout our previous posts.
This woman, let’s call her Abigail, had a knee injury a couple of years ago. At that time, the knee pain got pretty bad. It definitely interfered with her function. She wanted to go jogging, but that caused the pain to flare up, so she stopped doing it. Sometimes she even had trouble walking. She had a really hard time getting up and down off the floor with her young children, and it interfered with her enjoyment of spending time with them. She went to her doctor, who diagnosed it and referred her to a physiotherapist (PT). The PT taught her how to strengthen her quadriceps to put less strain on her knee. She had custom shoe inserts made to support her flat feet (which can cause her knees to go inward, and was thought to be contributing to the pain). She iced her knee and took anti-inflammatories only when the pain got really bad, thinking that she should avoid taking too many meds. She wore a knee brace for a while, because she felt scared to do things without it on. All these things seemed to help, and she felt good that she had a few strategies, but it took months until the pain gradually went away.
Now fast forward a couple of years. Abigail is in better shape overall, and her knee hasn’t been bothering her, unless she does too many squats. She likes to go to a zumba class a couple of times per month. She wants to be able to go jogging, because she has enjoyed that in the past. She’s a little worried that her knee might bother her, but she wants to try it. She starts a running routine with some co-workers, taking it easy at first and gradually building up, with a goal of reaching 30 minutes. She registers for a 5km fun run, hoping she’ll actually be able to run it. The first few weeks of training, her knee feels fine. She’s pleasantly surprised, but still careful.
When she gets to a point where she’s running 20 minute intervals, the knee pain is suddenly back. It’s relatively mild at this point, but it’s got her attention. She knows she doesn’t want to go back to the moderate/severe pain that affected her so much two years ago.
This time, she sees an occupational therapist and a physiotherapist who both specialize in pain. Her health care team explains some theories and science around pain.
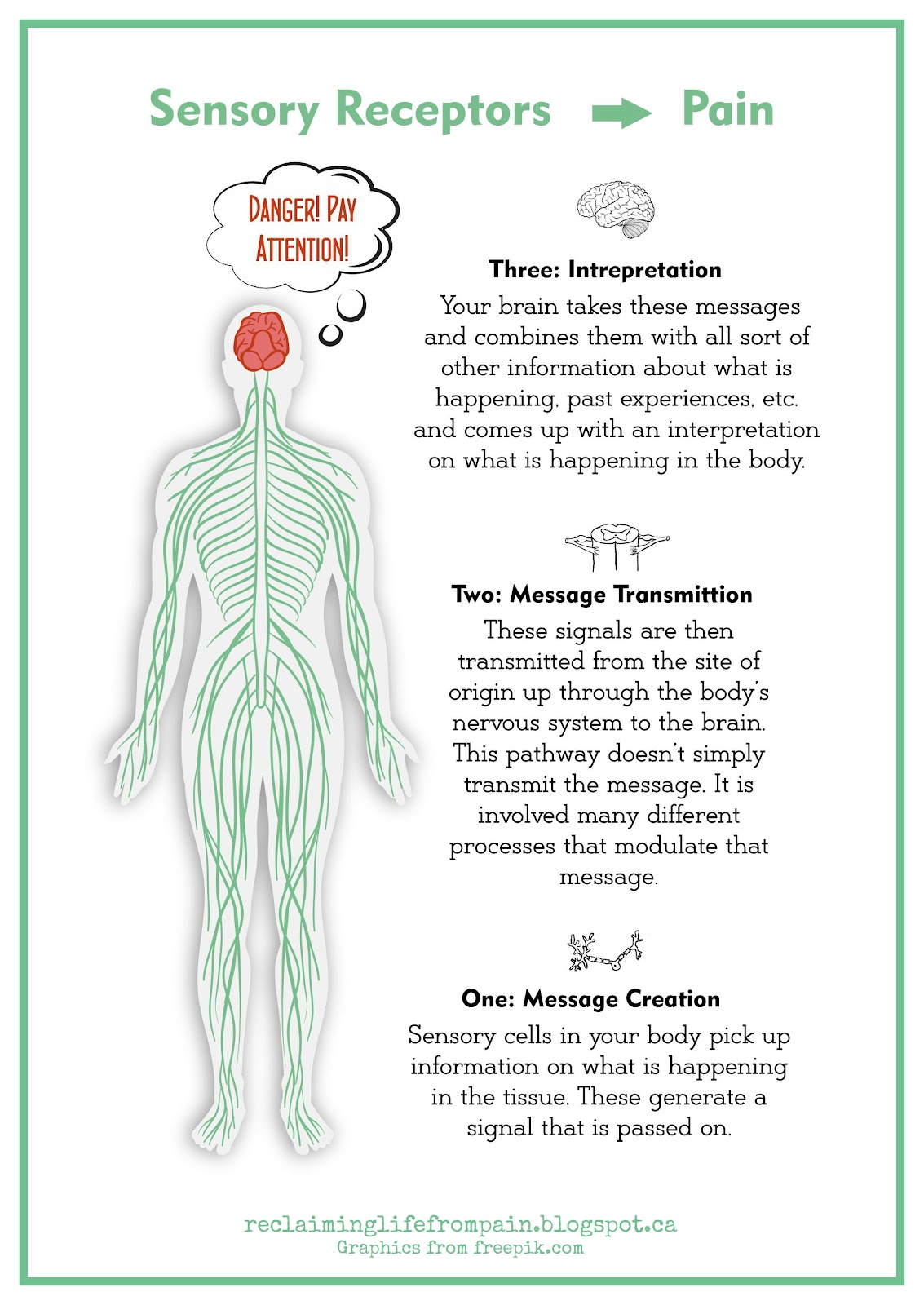
1. The “Pain Alarm” (see this post)
- The pain alarm can be useful, so it is probably telling her something.
- Since the pain clearly started when she began to run 20 minutes at a time, she thinks it’s probably telling her she’s pushing herself too hard, too fast.
- But if she blindly listens to that alarm, or misinterprets what it’s telling her, and she stops moving completely, it will likely get worse.
2. Pain related fear and avoidance (see the diagram on this post)
- If she stops doing activities that can hurt (like running, zumba, or playing with her kids), the decreased activity could actually make things more difficult and painful. This in turn could increase her avoidance of these tasks, creating a cycle that results in decreased functioning.
- If she completely ignores what her body is saying, and continues trying to increase her running endurance by trying harder and harder to push through the pain, well, that could potentially cause serious pain. Which would lead to avoiding activities because her knee truly can’t tolerate them. This in turn could lead to more fear, and more avoidance, and more pain.
3. “Safety in Me” vs “Danger in me” (see this website)
- There is value in anything that helps build her confidence in her body’s ability to move without causing her pain to get worse.
So basically, Abigail knows she has to pay attention to the acute pain “alarm.” She needs to find the balance where she continues to do activities, but doesn’t overdo it. Understanding these concepts, she works with her health care team to explore how her new knowledge applies to her situation, and develops some strategies:
- She knows that she needs to keep moving, but aims to “fly under the radar” (see last post) of pain, meaning that she will do movements that bring her just to the point of discomfort, but not past it into pain. Basically, she wants to stay in the pushing-herself-but-safe zone.
- With that in mind, she scales back on running, but doesn’t stop. She knows that when she was running for 16 minutes, her knee pain didn’t flare up. So she decides to go back down from 20 minutes to 16, and stay there for a couple of weeks. She plans to increase her time only if she feels the pain is well under control.
- She decides to replace Zumba classes with water aerobics for a while, to give her the chance to focus on running. She realizes that both running and Zumba involve impact on her joints, and decides she needs to choose one to focus on. She wants to increase her running endurance, so that's the one she chooses.
- She learns different exercises from her physiotherapist. This time the exercises are more personalized to the specific reason for her knee pain.
- She ices her knee and takes anti-inflammatories any time she feels the pain and swelling coming, instead of trying to be “tough” and taking meds only when she can’t take the pain anymore. She knows she wants to keep the inflammation at bay so she can keep moving.
Abigail finds great success in this plan. She’s absolutely thrilled that she was able to do it, and is so glad that she didn’t stop running when the pain first started. She’s also glad she took the pain seriously and came up with a plan. She’s grateful for all of the pain theory that she was able to build into her plan. The best part - in another month, she’s able to run the 5 km fun run without experiencing knee pain!
Acknowledgments:
Diagram by Reclaiming Life. Graphics from freepik.com