"If we’re in pain, it's changes in our total body that have lead to chronic pain, but it is changeable." - David Butler (2015)
At the end of our last post we talked about how pain treatment is evolving and growing as knowledge of pain increases. We described some neurophysiology concepts in that post, and how they relate to pain. Now let’s go one step deeper and look at an overall approach and some specific treatments that apply these concepts to clinical practice.
The neuromatrix approach described by Moseley (2003) leads to a clinical framework that involves using this knowledge of brain mechanisms to change the experience of pain. Research into neuroplasticity has opened the door to the idea that our brains can, and do, change throughout our entire lives. The great thing about this is it creates new possibilities in the treatment of pain.
All of these ideas are based on some common themes:
- Many areas of our brain work together as part of the pain response. The network that makes up this response is unique to each individual.
- Pain is an alarm telling us that something is wrong - but the alarm can malfunction. It can respond to the wrong type of information, or require less activation of the network to produce a pain response.“Smaller and seemingly less relevant inputs are sufficient to...produce pain” (Moseley, 2003, p. 4).
- If we can decrease the threat value of the signals our brain receives, or allow more of the network to be activated before the pain response is triggered, we can decrease the pain (Moseley, 2003).
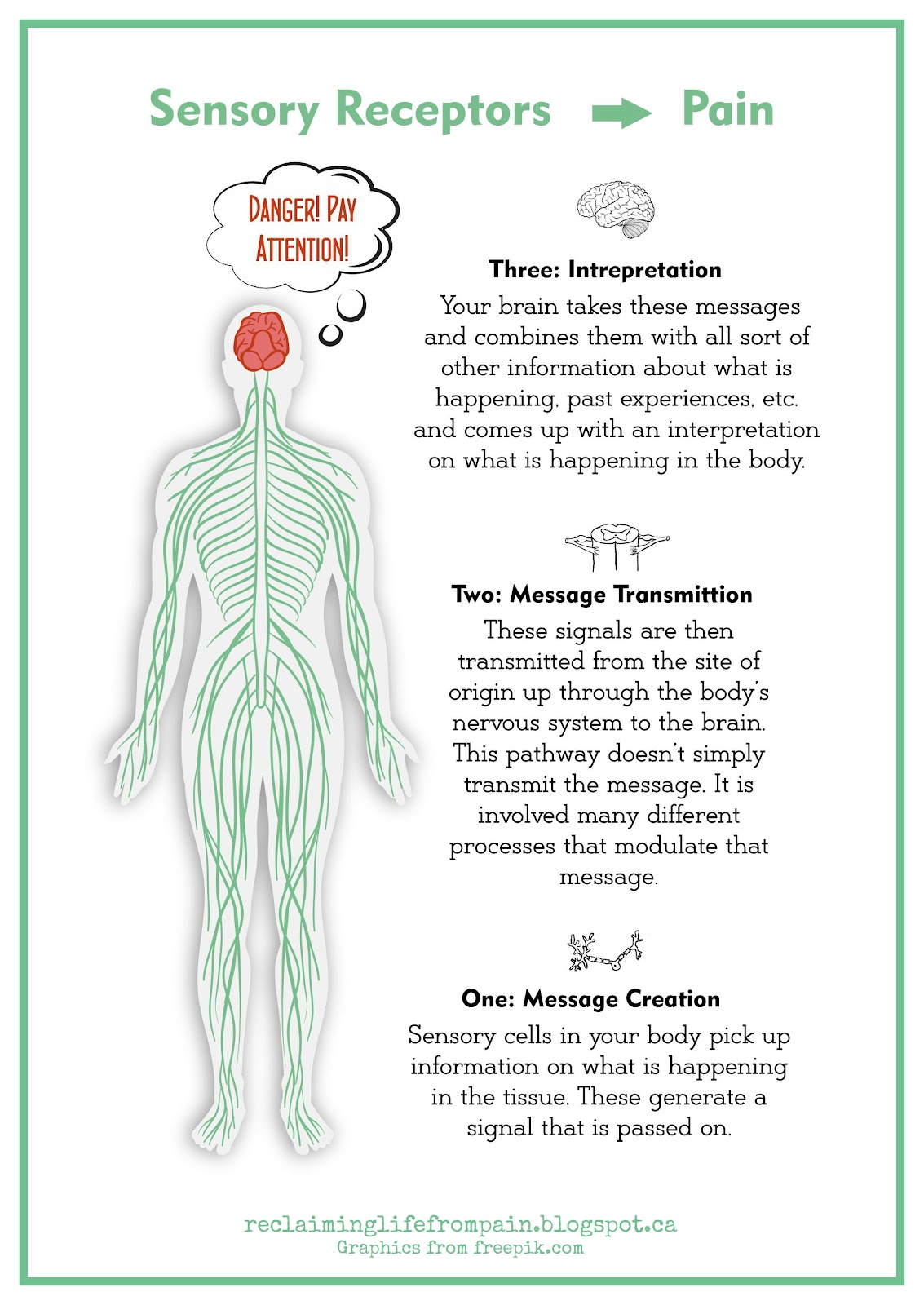
Moseley (2003) explained three steps to treatment based on these concepts. Today, we’ll examine each step and how a variety of treatment ideas could be incorporated into the process he described.
1. An initial step in treatment involves reducing the threatening input and/or the threat value the brain assigns to these signals. The idea is that if the signals coming from the body are decreased or interpreted as less of a threat, then the alarm doesn’t need to sound as loud. There are several ways to achieve this. One way is by fixing physical issues in order to reduce the actual input. This can be done through manual therapy, exercises, heat/ice as appropriate, pain medications, etc. Another approach is to reduce the threat value of the inputs. This can be done by things like education about pain, and techniques that calm your nervous system like relaxation, deep breathing, and even laughter yoga.
2. The next step is to figure out how to activate components of the “neuromatrix” without triggering pain. Like we talked about last time, the neuromatrix is a network comprised of different areas and processes within the brain. When enough of the network is activated the pain response is triggered. The goal with this step is to activate some components of this network without activating the pain response. Some examples of ways to do this include:
- visualization (imagining pain free movement)
- breaking activities down into simple movements
- reducing the physical demand of a task
- changing the way tasks are done
- changing the context surrounding tasks
- changing the language we use to decrease the “threat” associated with a particular movement
3. Then, the next step is to gradually increase how much of the neuromatrix is activated, so that more and more of it can be activated without resulting in pain. The key to achieving this without causing flare ups is to be aware of the threshold (how much of the neuromatrix can be activated without pain), and very gradually increase that threshold. One way to conceptualize this is the idea of flying under the radar, as described in the graphic below. The idea is to avoid triggering enough of the neuromatrix to cause a flare-up, and gradually push the limits. This will increase how much of the neuromatrix can be activated before a flare up is triggered.

Modern science and knowledge about the brain and nervous system has opened up a variety of treatment options. Treatment can be done in several different ways, depending on the individual’s needs, and the approach can change over time as needed. Note, we have to be careful attributing everything to the brain. The brain clearly plays a huge role in pain, but human beings are vastly complex, and so is pain. In order to understand pain, clinicians need to understand “several domains...neuroscience, immunology, endocrinology, psychology, sociology, and philosophy”. (First-person neuroscience and the understanding of pain. Thacker and Moseley. 2012). We would like to suggest that because so many factors contribute to pain, there is hope that all of these factors can be used to change pain. Even though we don’t have a cure for chronic pain yet, we do have solutions; methods to reduce and manage it, and learn to function better.
Acknowledgement:
References:
Butler, D. via Arthritis Victoria. (2015, August 3). Treating Pain Using the Brain - David Butler [Video File]. Retrieved from https://youtu.be/4ABAS3tkkuE on April 22, 2016.
Moseley, G.L. (2003). A pain neuromatrix approach to patients with chronic pain. Manual Therapy, 8(3), 130-140.
Moseley, G.L. (2003). A pain neuromatrix approach to patients with chronic pain. Manual Therapy, 8(3), 130-140.
Thacker, M.A., & Moseley, G.L. (2012). First-person neuroscience and the understanding of pain. The Medical Journal of Australia, 196(6), 410-411.
Melzack, R. (2001). Pain and the neuromatrix in the brain. Journal of Dental Education, 65(12), 1378-1382.
Melzack, R. (2001). Pain and the neuromatrix in the brain. Journal of Dental Education, 65(12), 1378-1382.